
{kind=link}
Is that suddenly worse rash a flare of eczema, or an infection that needs a doctor today?
This matters because the steps you take are different and the wrong move can let an infection spread.
A flare usually stays itchy, dry, and familiar. Infection brings new pain, warmth, yellow crusts or pus, and sometimes fever.
Read on to learn the quick red flags, simple home checks, what to try safely, and when to get same-day medical care.
Key Differences to Recognize an Eczema Flare vs a Skin Infection

When eczema suddenly looks worse, you’re probably asking yourself whether this is a flare or something more serious. Eczema flares stick to a familiar script: itching, dryness, redness spreading slowly across patches you’ve seen before. Infected skin doesn’t follow that pattern. Pain starts showing up where itch used to dominate. The skin feels hot. Crusts turn yellow or honey colored instead of clear or white. You might see bumps filled with pus, red streaks radiating outward, swelling that feels warm when you touch it. Those signs point toward infection, not just a typical flare.
Systemic symptoms make things clearer. Fever over 100.4°F, swollen lymph nodes close to the rash, chills, feeling generally lousy. Simple flares don’t usually come with that package, but infections do. If your child goes to bed with manageable eczema and wakes up with a fever and a rash that’s visibly worse, that rapid shift suggests infection has taken hold.
| Feature | Eczema Flare | Infection |
|---|---|---|
| Itching | Intense, dominant symptom | Often reduced or replaced by pain |
| Pain | Minimal or absent | Sharp, tender, worsening |
| Redness Pattern | Patchy, slow spread within known areas | Rapid spread, streaking, warm edges |
| Crust Type | Clear, white, or dry flakes | Yellow, honey-colored, or green-tinged |
| Discharge | Mild weeping or none | Pus, thick drainage, foul odor |
| Systemic Signs | Rare | Fever ≥ 100.4°F, swollen lymph nodes, chills |
How Symptoms Progress Over Time in Flares vs Infections

The way symptoms change over hours and days often tells you what you’re dealing with. Eczema flares build gradually. Your skin gets drier first, then itchier, then redder over several days, especially after you’ve been exposed to a trigger like soap, stress, or dry air. You scratch more at night, wake up with scaly patches, maybe notice mild oozing if you’ve rubbed spots raw. But the discomfort stays centered on itch and tightness.
Infection shows up differently. A patch that was simply itchy yesterday becomes sharply painful today. Warmth spreads outward from the center. Instead of clear fluid, you see cloudy or yellow pus collecting under the surface or crusting over in thick, sticky layers. Bacterial infections, especially staph, can produce honey colored crusts that feel tacky and look like dried syrup. When pain takes over where itch used to be and the skin feels hot instead of just irritated, bacteria have likely moved beyond surface colonization into active infection.
Viral and fungal infections have their own timelines. Eczema herpeticum, caused by herpes simplex virus, erupts fast. Within 24 to 48 hours, clustered blisters appear that look punched out, weep clear fluid, and hurt more than they itch. Fungal infections move slower, expanding as scaly rings with raised edges over weeks, sometimes forming small pustules at the border. If you’re seeing spreading circles or sudden painful blisters rather than the familiar dry, itchy, scratch cycle, consider infection.
Eczema Infection Warning Signs That Require Prompt Care

Some changes demand same day or urgent evaluation because they signal that infection is moving beyond the skin’s surface or spreading rapidly. Red streaks extending from the rash toward the nearest lymph nodes? That’s lymphangitis, bacteria traveling through lymph channels, and it requires immediate antibiotic treatment.
Watch for these red flags:
Fever of 100.4°F (38°C) or higher accompanying worsening skin symptoms. Red streaks radiating from the rash. Swollen, tender lymph nodes in the neck, armpits, or groin near the affected skin. Rapidly spreading redness that doubles in size within 24 hours. Chills, malaise, or feeling flu like while the rash worsens. Pus filled blisters covering large areas or appearing near the eyes, face, or groin.
Common Types of Infections That Occur on Eczema Prone Skin
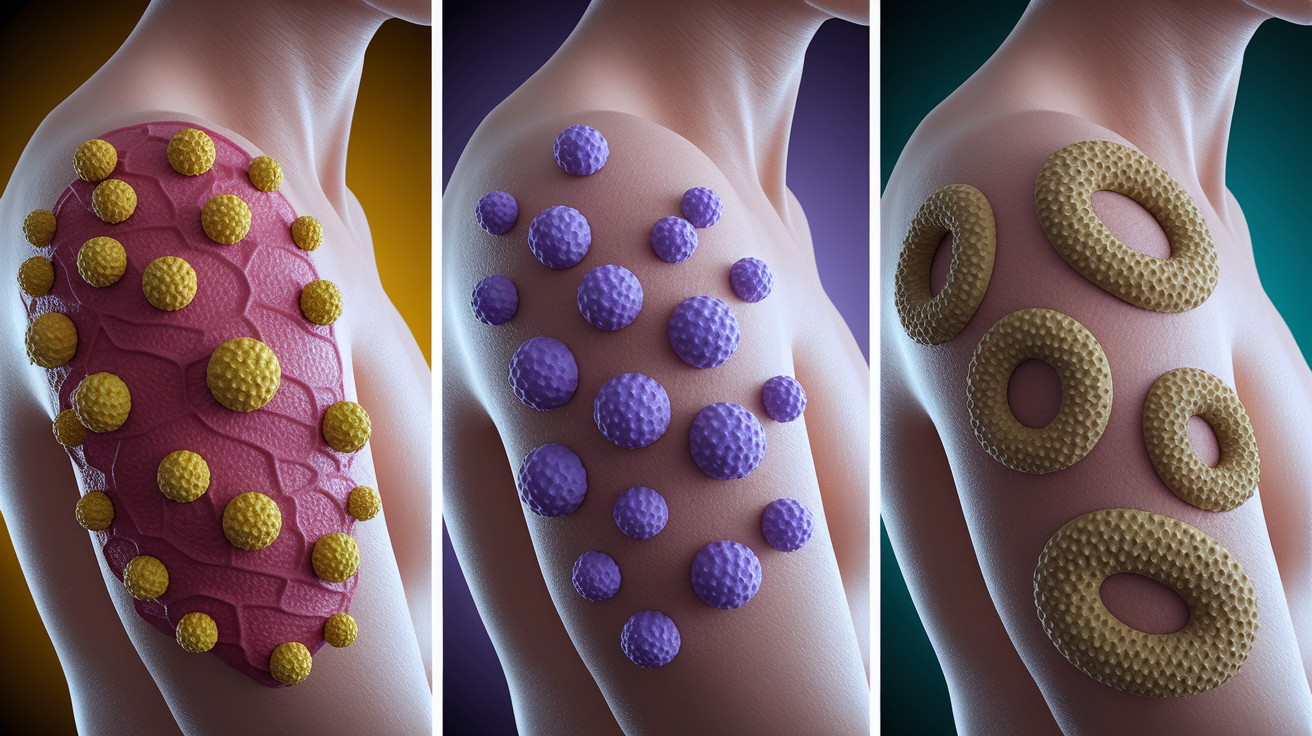
Three main categories of pathogens take advantage of eczema’s weakened skin barrier: bacteria, viruses, and fungi. Each leaves a recognizable pattern. Knowing what to look for helps you describe symptoms clearly when you contact a clinician.
Bacterial Infections on Eczema
Staphylococcus aureus is the most common bacterial colonizer of eczema skin, living on up to 80 to 90% of active lesions without always causing overt infection. When it does break through, it typically causes impetigo, shallow sores topped with golden yellow crusts, or cellulitis, a deeper infection marked by spreading warmth, swelling, and pain. MRSA, a methicillin resistant form of staph, produces similar symptoms but often shows up as boils or abscesses filled with pus. These purulent pockets feel firm, hot, and extremely tender, and they require antibiotics chosen specifically to target resistant strains.
Viral Outbreaks on Eczema
Herpes simplex virus can cause eczema herpeticum, a serious complication that looks like clusters of small blisters or punched out erosions scattered across eczema patches. The blisters weep clear fluid, crust over quickly, and hurt more than typical eczema ever does. This infection can spread fast and, in severe cases, become systemic. It requires urgent antiviral treatment, usually oral acyclovir started as soon as the pattern is recognized. Eczema herpeticum is less common than bacterial infections but clinically significant because delays in treatment can lead to complications.
Fungal Overgrowth on Eczema
Dermatophytes (ringworm fungi) and Candida yeast occasionally infect eczema skin, especially in warm, moist areas like skin folds. Fungal infections present as red, scaly patches with well defined borders that expand slowly outward in rings. You might see small pustules at the advancing edge or satellite lesions nearby. Candida often causes bright red rashes with satellite papules and a raw, shiny surface. These infections respond to antifungal creams or oral medication but won’t improve with antibiotics or standard eczema treatment.
Why Eczema Skin Gets Infected More Easily
Healthy skin acts as a physical and chemical fortress. Eczema dismantles that defense in multiple ways. The outermost layer, the stratum corneum, loses integrity because of defects in proteins like filaggrin, which normally hold skin cells together and retain moisture. Cracks form, water escapes, and allergens, irritants, and bacteria slip through gaps that shouldn’t exist.
People with eczema also produce fewer antimicrobial peptides, the skin’s natural antibiotics. Without enough of these defensive molecules, bacteria like Staphylococcus aureus colonize more heavily and form biofilms, sticky protective layers that shield bacteria from the immune system and allow them to thrive. Staph doesn’t just live passively on eczema skin. It actively worsens inflammation by releasing enzymes and toxins that trigger immune overreactions and further damage the barrier.
Scratching completes the cycle. Every time fingernails break the surface, they inoculate deeper layers with whatever bacteria, viruses, or fungi are present on the skin or under the nails. Open wounds become entry points for pathogens that would otherwise remain harmless surface colonizers. The cycle repeats: inflammation causes itch, itch causes scratching, scratching breaks skin, broken skin gets infected, infection worsens inflammation.
Defective skin barrier proteins allow pathogen entry. Reduced antimicrobial peptides fail to suppress bacterial growth. Scratching introduces surface microbes into deeper tissue. Staph biofilms shield bacteria and amplify inflammation.
How Doctors Diagnose Flare vs Infection

Clinicians start with a careful look at the rash’s appearance, distribution, and associated symptoms. They check for warmth by pressing the back of their hand against the skin, compare the affected area to surrounding normal skin, and ask about pain versus itch. Yellow crusts, pus, red streaks, and rapid overnight changes all shift suspicion toward infection. Fever, swollen lymph nodes, and worsening despite usual eczema care further support that diagnosis.
When the picture isn’t clear or symptoms don’t respond to initial treatment within 48 to 72 hours, clinicians order tests. A bacterial culture swab from pus or crusted areas identifies the organism and tests which antibiotics will work. PCR testing can detect herpes simplex virus quickly when eczema herpeticum is suspected. Fungal cultures or potassium hydroxide (KOH) preparations help confirm ringworm or yeast infections. These tests take time. Bacterial cultures often need 48 hours, fungal cultures longer. But they guide precise treatment when empiric therapy fails.
| Test | When It’s Used |
|---|---|
| Bacterial culture and sensitivity | Purulent discharge, worsening despite antibiotics, suspected MRSA |
| Viral PCR or culture | Clustered painful blisters, suspected eczema herpeticum |
| Fungal KOH prep or culture | Ring-shaped rash, scaly borders, no response to steroids or antibiotics |
| Clinical examination alone | Classic impetigo with honey crusts, clear cellulitis with fever |
Treatment Differences: Eczema Flare vs Confirmed Infection

When you’re managing a flare without infection, the goal is to calm inflammation, restore the skin barrier, and stop the itch scratch cycle. That means applying thick emollients at least two to three times daily, using prescribed topical corticosteroids or calcineurin inhibitors as directed, and sometimes adding wet wrap therapy, damp layers of cloth over medicated skin, to lock in moisture and medication overnight. Oral antihistamines can help with nighttime itching, though they don’t treat the underlying inflammation.
Infected eczema requires different tools. Localized bacterial infections with small areas of impetigo often respond to topical antibiotics like mupirocin applied two to three times daily for five to seven days. When infection spreads more widely or causes cellulitis, oral antibiotics become necessary. First line choices for typical staph and strep include cephalexin or dicloxacillin. If MRSA is suspected, because of local resistance patterns, purulent abscesses, or failure of initial antibiotics, clinicians switch to agents like trimethoprim sulfamethoxazole, doxycycline, or clindamycin. Eczema herpeticum demands urgent oral antivirals, typically acyclovir, started as soon as the diagnosis is made to prevent systemic spread. Fungal infections respond to topical antifungals for mild cases or oral agents like fluconazole for extensive involvement.
Steroid use during active infection requires clinical judgment. Some clinicians pause or reduce topical steroids until bacterial or viral infections are controlled, because steroids can suppress local immune defenses and allow infections to worsen. Others continue steroids at lower potency while treating the infection simultaneously, especially if inflammation is severe. If you’re unsure whether to keep using your steroid cream, contact your clinician rather than guessing.
Flares without infection get emollients, topical steroids, wet wraps, antihistamines. Localized bacterial infection gets topical mupirocin. Widespread bacterial infection or cellulitis gets oral antibiotics like cephalexin, dicloxacillin, or MRSA active agents. Eczema herpeticum gets urgent oral antivirals like acyclovir. Fungal infection gets topical or oral antifungals depending on extent.
When to Seek Medical Care for Worsening Eczema

Not every worsening rash requires urgent attention, but certain patterns and timelines do. If eczema that usually responds to your routine suddenly doesn’t improve after 48 to 72 hours of intensified moisturizing and prescribed treatment, contact your clinician. When pain replaces itch, when crusts turn yellow or green, when red streaks appear, or when swelling increases rapidly, those changes suggest infection and warrant same day evaluation.
Children with eczema who develop fever and a rash that’s visibly spreading need assessment the same day, especially if lesions appear near the eyes, face, or in skin folds where infection can worsen quickly. Swollen lymph nodes near the rash, chills, or feeling generally unwell alongside skin changes all indicate possible systemic involvement. Don’t wait to see if these symptoms resolve on their own.
Contact a clinician or seek care promptly if you notice:
Fever of 100.4°F (38°C) or higher with worsening skin symptoms. Spreading redness or swelling that doubles in size within 24 hours. Pus, thick yellow or green drainage, or a foul odor from the rash. Red streaks extending from the affected area. Swollen, tender lymph nodes in the neck, armpits, or groin. Rash near the eyes, face, hands, or groin that’s rapidly worsening or painful.
Preventing Infection During and Between Eczema Flares

The best defense against skin infections is keeping the eczema barrier as intact as possible. That starts with aggressive, boring basics. Moisturize multiple times daily with thick emollients, especially right after bathing when skin is still damp. Keep fingernails trimmed short and clean to reduce bacterial load and limit damage from scratching. Wash hands frequently, especially before applying creams or touching active eczema patches, and don’t share towels, razors, or washcloths with others.
Cover flares with soft clothing when practical to reduce direct contact with environmental bacteria and to discourage unconscious scratching. Use pump dispenser bottles for lotions and creams instead of dipping fingers into communal tubs, which can introduce bacteria into the product. If someone in your household has an active staph or herpes infection, practice careful hygiene. Separate towels, frequent hand washing, and avoid skin to skin contact with open lesions to reduce transmission risk.
For people with recurrent staph infections, clinicians sometimes recommend a decolonization plan. This might include a short course of topical antibiotic ointment applied inside the nostrils (a common staph reservoir), antiseptic body washes, and household measures like laundering towels and sheets in hot water. These strategies aim to reduce the bacterial load on skin and in the environment without relying on continuous oral antibiotics.
Daily prevention steps include:
Apply thick emollients at least two to three times daily, always after bathing. Trim and clean fingernails weekly. Wash hands before applying creams or touching eczema patches. Use pump dispensers for shared skin care products. Don’t share towels, razors, or washcloths. Cover active flares with soft, breathable clothing when possible.
Safe Use of Dilute Bleach Baths
Dilute bleach baths can reduce bacterial load on eczema skin and lower infection risk when used correctly. The typical regimen is about 1/4 cup (60 mL) of regular household bleach, 6% sodium hypochlorite, the kind used for laundry, added to a full bathtub of water, roughly 40 gallons. Soak for five to ten minutes, twice weekly, then rinse off with plain water and apply emollients immediately. Never pour bleach directly onto skin, keep it away from eyes, and don’t use bleach baths during active open wounds or severe flares without clinician guidance. This is a maintenance strategy, not an acute infection treatment.
Final Words
In the action, this post showed how to tell a red, itchy patch is a flare or likely an infection. You saw key signs, how symptoms evolve, common infection patterns, when to get checked, and simple prevention steps.
Watch itch turning into pain, spreading warmth, pus or honey-colored crusts, fever, or red streaks. Use the comparisons and timelines here to help decide on eczema flare vs infection.
Write down when symptoms started, what helps, and any treatments you try so your clinician gets a clear story. You’ve got a plan and can get help when needed.
FAQ
Q: How to tell the difference between eczema and bacterial infection?
A: The difference between eczema and bacterial infection is that eczema is usually very itchy, dry, scaly and slowly worse, while infection brings increasing pain, spreading warmth, pus or honey-colored crusts—see a clinician if those appear.
Q: What is the 3 minute rule for eczema?
A: The 3 minute rule for eczema is applying moisturizer within three minutes after bathing to lock in moisture. Pat skin dry, use a gentle emollient, and repeat after every wash.
Q: How do I know eczema is infected?
A: You know eczema is infected when itch becomes increasing pain, the area gets warmer or spreads, you see pus or yellow/honey crusts, red streaks, swollen lymph nodes, or you have a fever—seek care promptly.
Q: Will antifungal cream make eczema worse?
A: Antifungal cream will not usually make eczema worse, but it won’t help if the rash is plain eczema, not a fungus. Use antifungals when a fungal infection is likely or after clinician advice.